



The FDA has NOT Banned Trans Fats! Traditional Saturated Fats like Coconut Oil Continue to Shine for Alzheimer’s Disease but are Condemned by U.S. Dietary Advice

The FDA has NOT Banned Trans Fats! Traditional Saturated Fats like Coconut Oil Continue to Shine for Alzheimer's Disease but are Condemned by U.S. Dietary Advice
It has been widely reported in the Alternative Media this month that the FDA has banned trans fats, and that they will no longer be allowed in foods starting December 22, 2023. Please note: if you believe that the FDA always tells us the truth because they want to protect us, ...
The Evidence of Coconut Oil's Superiority Over Drugs in Destroying Pathogens Continues to be Published in Peer-Reviewed Journals
The U.S. Government's official position on coconut oil today continues to be that it is dangerous for your health, and that you should either avoid it altogether, or only consume very modest amounts. The reason that has been given for this official position for over four decades now, is because it ...
Study: Virgin Coconut Oil Protects Neuronal Damage and Mortality after a Stroke Incidence
Researchers from Japan and the Philippines have just published a new study conducted on "stroke-prone" hypertensive rats that indicate Virgin Coconut Oil can help prevent neuronal damage and deaths due to strokes. Given the fact that we have seen an astounding 100,000% increase in strokes recorded in VAERS (Vaccine Adverse Events ...
Another Phase 3 Trial Failure to Develop an Alzheimer's Drug Shows Why Virgin Coconut Oil is Needed to Prevent Dementia
After more than a decade of failed drug trials and $billions lost in research to try and bring an Alzheimer's drug to market, maybe the pharmaceutical industry is finally ready to admit that they don't really understand what causes Alzheimer's disease. It was announced earlier this week that Roche had failed ...
FDA Food Police want to Dictate What Foods are Healthy in New Guidelines Criminalizing Traditional Fats Like Butter and Coconut Oil
The criminal U.S. Food and Drug Administration (FDA) yesterday published new proposed rules dictating when food products can have the word “healthy” on their packaging and when they cannot. The problem is that you should not trust the FDA to tell you which foods are healthy and which foods are not, ...Coconut Oil
Your source for research and news on the health benefits of coconut oil.

A coconut oil truck is a common sight on the roadways in the Philippines. Unlike the US where coconut oil has been hard to find in recent years, coconut oil has been a big part of the diet in the Philippines and many other tropical cultures for thousands of years.
CoconutOil.com is the Internet’s oldest resource for published research on the health benefits of coconut oil. Beginning in the year 2000, we have been the main source of information linking to peer-reviewed research on coconut oil as well as publishing coconut oil testimonials showing how coconut oil has changed people’s lives!
Coconut oil is an edible oil that has been consumed in tropical places for thousands of years. Studies done on native diets high in coconut oil consumption show that these populations are generally in good health, and don’t suffer as much from many of the modern diseases of western nations where coconut oil is seldom consumed anymore.
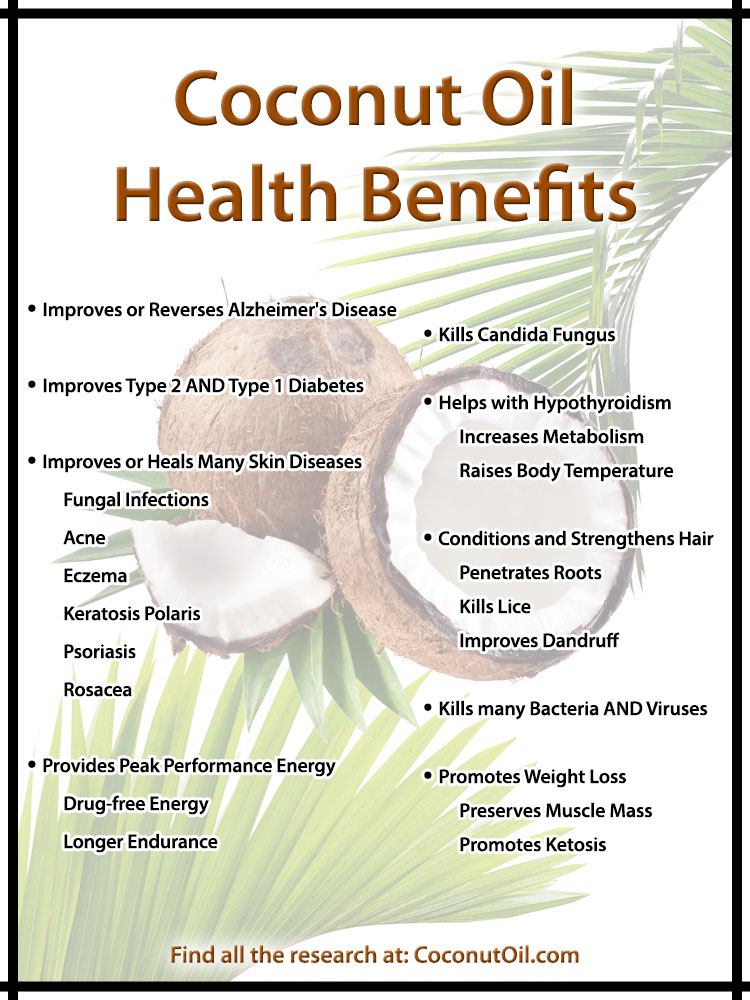
Coconut Oil Health Benefits
So how are people using coconut oil? What are some of the health benefits of coconut oil being reported? Some of the most recent research has come from people suffering from Alzheimer’s disease, with reports of people improving or even reversing the effects of Alzheimer’s by using coconut oil, as drug trials on Alzheimer’s drugs continue to fail. Alzheimer’s is now seen as a type 3 form of diabetes, and for years we have seen positive results from people with both type 1 and type 2 diabetes in using coconut oil. We have also seen a lot of reports of coconut oil health benefits from those suffering from hypothyroidism, as coconut oil helps boost metabolism and raise body temperatures to promote thyroid health. Restricting carbohydrates and increasing coconut oil in the diet has also led many to report losing weight with coconut oil. Candida sufferers also report health benefits with coconut oil as research now confirms, and those suffering from various skin diseases are also seeing tremendous health benefits by applying coconut oil directly on the skin. The benefits of coconut oil for healthy hair are also well known, and other healthy benefits of coconut oil included fighting off bacterial infections and viruses. Coconut oil is also increasingly being seen to benefit athletes and fitness trainers giving them an advantage in sustaining energy levels longer without drugs or stimulants.
Coconut Oil Research
While some people falsely accuse coconut oil of being a “fad,” the fact is that it is a traditional oil that has been consumed for thousands of years in tropical cultures, and the research on the health benefits of coconut oil has existed for a very long time. Lauric acid, for example, has a long history of use in combating pathogens, and this research has been around for more than 50 years. Coconut oil is nature’s richest source of lauric acid. So while we do publish a lot of people’s experiences with coconut oil, the evidence is not strictly anecdotal. We have a very extensive section on this website dedicated to peer-reviewed studies on the health benefits of coconut oil that are accessed primarily through Pubmed. This section is updated frequently as new research is published.

Virgin Coconut Oil: How it has changed people’s lives, and how it can change yours! Over 100 testimonies and 85 recipes.
Coconut oil was once prevalent in western countries like the United States. With a long shelf life and a melting point of 76 degrees, coconut oil was a favorite in the baking industry. But a negative campaign against saturated fats in general, and coconut oil in particular, led to most food manufacturers abandoning coconut oil in recent years in favor of hydrogenated polyunsaturated oils that come from the main government-subsidized cash crops in the US, particularly corn and soy. These hydrogenated oils contain trans fatty acids. The polyunsaturated oils were not a big part of the diet of previous generations, so how has the health of Americans changed now that polyunsaturated oils are for the most part all one finds on supermarket shelves across the US? We encourage you to take an honest look at the research presented on this website, and consider the “other side” of the story, whether it be coconut oil, saturated fats, cholesterol, or the new vegetable oils!
Coconut Oil Testimonies
The CoconutDiet.com website contains the Coconut Diet Forums, which is a compilation of discussions of people discussing the health benefits of coconut oil over a 10+ year period. This was the first Internet discussion group started back in 2001 by Brian Shilhavy, while still living in the Philippines at the time. There are over 17,000 messages covering a wide range of coconut oil health topics, with contributions from many of the early leaders of the coconut oil movement that brought coconut oil back into prominence in the early 2000s. There are currently over 100,000 subscribers.
With today’s social media, however, you will find many of the the most current testimonials about the health benefits of coconut oil by following the Coconut Health Twitter account, the top Twitter account covering the health benefits of coconut oil, or by following the discussions on the Coconut Health Facebook Page, the top Facebook page discussing the health benefits of coconut oil.
Coconut Oil News
You can find all the latest coconut oil news published throughout the Internet at Health Impact News, in the Coconut Health section. Brian Shilhavy is the editor of Health Impact News, and he tracks the news throughout the Internet each day to cover the top stories related to the health benefits of coconut oil, as well as other alternative health news. Published studies that appear in peer-reviewed journals will be logged here, on CoconutOil.com, on our peer-reviewed coconut oil research page. We have also added a coconut oil news section here on CoconutOil.com that can be tracked via an RSS reader to stay up to date on all the latest news regarding coconut oil.
What is the Best Type of Coconut Oil?
There are many different types of coconut oil currently in the market, using a variety of different terminology by the vendors to describe their product. We sort it all out for you here: What Type of Coconut Oil is Best? How to Choose a Coconut Oil.
Coconut Oil Recipes
FreeCoconutRecipes.com has the largest collection of coconut recipes found anywhere on the Internet. There are recipe sections for Coconut Oil recipes, Gluten Free Coconut Flour recipes, Coconut Cream Concentrate recipes, and many others. There are hundreds of coconut recipes, all kitchen tested and submitted by coconut users who love coconut. There are many cooking and baking video demonstrations as well, helping you to learn how to use coconut oil in your everyday cooking and baking. Here is one video overview showing many of the ways one can use coconut oil in a healthy diet:
Coconutoil.com includes the original body of research on coconut oil that was published in 2000, originally at coconut-info.com, and started the current coconut oil revolution in the U.S. and around the world! We continue to be the leading website on the most current research on the health benefits of coconut oil.
 The FDA has NOT Banned Trans Fats! Traditional Saturated Fats like Coconut Oil Continue to Shine for Alzheimer's Disease but are Condemned by U.S. Dietary Advice
The FDA has NOT Banned Trans Fats! Traditional Saturated Fats like Coconut Oil Continue to Shine for Alzheimer's Disease but are Condemned by U.S. Dietary Advice The Evidence of Coconut Oil's Superiority Over Drugs in Destroying Pathogens Continues to be Published in Peer-Reviewed Journals
The Evidence of Coconut Oil's Superiority Over Drugs in Destroying Pathogens Continues to be Published in Peer-Reviewed Journals Study: Virgin Coconut Oil Protects Neuronal Damage and Mortality after a Stroke Incidence
Study: Virgin Coconut Oil Protects Neuronal Damage and Mortality after a Stroke Incidence Another Phase 3 Trial Failure to Develop an Alzheimer's Drug Shows Why Virgin Coconut Oil is Needed to Prevent Dementia
Another Phase 3 Trial Failure to Develop an Alzheimer's Drug Shows Why Virgin Coconut Oil is Needed to Prevent Dementia FDA Food Police want to Dictate What Foods are "Healthy" in New Guidelines Criminalizing Traditional Fats Like Butter and Coconut Oil
FDA Food Police want to Dictate What Foods are "Healthy" in New Guidelines Criminalizing Traditional Fats Like Butter and Coconut Oil